

Physicians dislike being called "providers," but when do we stop calling patients "compliant"?
Names and frames matter for patient experiences.

If you’ve dealt with the American healthcare system for even a minute, it has probably occurred to you that there is a lot going on at the intersection of medicine, healthcare, and corporations.
People tell me their stories about gaslighting, and I often find myself pushing back on the idea that it’s alright to throw doctors under the bus, because there are critical systems in play that affect that happens in clinical settings.
But sometimes it is really difficult to feel sympathetic to physicians— as in this case below.
Fine, we get it. Gone are the days of our friendly family physician Marcus Welby, MD and our family doctor who hangs out their shingle and knows us from cradle to grave.
 - IMDb")
People have been writing about the medical-industrial complex for decades. This has meant changes to medical professions as physicians became more like corporate employees with the rise in HMOs in the 1980s. We doubled down on these trends after that with the continued rise of for-profit care in related sectors like health insurance. Alongside that, pharmaceuticals have become more prominent and, in the US, direct-to-consumer advertising is legal. Now we are pumping more private equity into healthcare. All of this momentum has steered medicine toward more of a business model—and we feel it at the pump, so to speak.
Somewhere in this business pipeline, physicians started getting called “providers.” Guess what? They don’t care for that at all.
In this article from the Annals of Internal Medicine (February 2026), the authors specifically pitch this as an ethical problem.
They tell us in laborious detail about the definitions and Latin origins of words like “patient,” “physician,” and “medicine.” My personal favorite is the part about the origins of “compassion” and how it is “essential to the patient-physician relationship” and “refers to supporting the patient in need and acting with and for the patient.”
Medical care is not a mere service. This is especially apparent in the origins of words associated with care. The Oxford English Dictionary defines the origins of the terms patient, physician, and medicine. Patient is from the Latin patiens, for one who suffers. This word refers to the vulnerability often brought on by illness. Doctor comes from the Latin docere (“to teach”). Physick originally meant medical treatment or remedy; one who practiced physick was a physician. By the 18th century, physic referred to the practice of medicine. Compassion comes from the Latin compassio, meaning “to suffer with.” Compassion is essential to the patient–physician relationship; it is not just empathy or kindness but refers to supporting the patient in need and acting with and for the patient. These words help convey the significance of what is at stake in medical care. (Sulmasy and Carney, 2026)
Words are important; I agree. But this sanitized notion of physicians as the compassionate gravitational center of the doctor-patient relationship, as the ones we can count on to “act with and for the patient”? Good grief: check out the comments here and see if people are buying into that.
One issue that is part of the problem, but unacknowledged in these kinds of publications, is that patients get different names too. These words we use around “users” or “consumers” of healthcare matter too.
Here is where we get into my having a beef that goes back years. Bear with me for a minute.
Back in 1997, Baby Karen wrote a PhD dissertation that was all about patient compliance. At the time, I was hot under the collar about a growing body of research that was focused on basically profiling “the compliant patient.” Starting in the 1960s, we searched for psychological, cognitive, and socioeconomic characteristics of patients that would predict how closely they followed medical recommendations— also framed as “acting in one’s own best interest,” which (eye roll) I have always taken as code for “acting rationally.” I felt like the questions getting asked in these fields were versions of: Are compliant patients just more educated? Smart? Motivated? Resourced?
In my study, I was asking: “how do doctors even try to assess how compliant patients are, given they only see them for short periods of time?” I shadowed endocrinologists in two diabetes clinics for most of a year, interviewing, videotaping, and calling patients at home afterwards to find answers. What I concluded was that “compliance” is not just about individual patient characteristics but also about doctor-patient interactions, the kinds of clinics and doctors involved, and the continuity of your care. How closely someone thinks you’re following a treatment plan is connected to social processes happening in healthcare.
After my dissertation, I even published this commentary with a physician, where we called for people to swap the term “compliance” (too paternalistic!) out for “adherence” (more patient agency!). That was 1999, and that little commentary has been cited about 500 times.
At first glance, this Annals paper appears in alignment with these ideas that patients have autonomy and should be partners in their care:
A physician should be a trusted confidant, counselor, advocate, and partner in times of need. Since Hippocrates, physicians have committed to putting the interests of patients first, utilizing their extensive knowledge, training, and experience to benefit patients and help keep them from harm. In contrast, providers provide. Business transactions need not focus on values or consider the interests of consumers before those of stockholders and owners.
But then I went and looked up how often “patient compliance” shows up in research articles these days, and I came up with this:
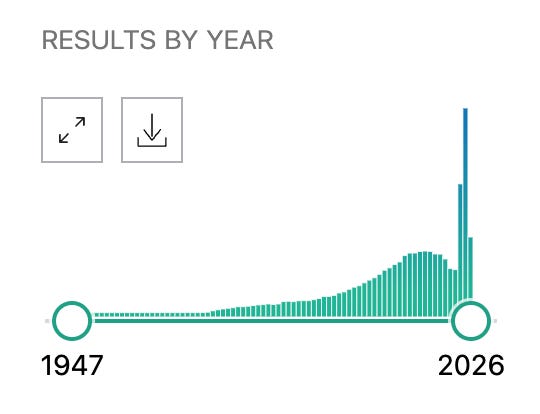
This is a search on the website www.pubmed.com, which is probably the major NIH-supported search engine for publications in medicine and public health. When I searched on “patient compliance,” this is the graph that came up to show how many articles with those key words were published in each year since 1947.
Keep in mind, back in 1997 I was already paying attention to what appeared, back then, as a big rise in studies on “compliance.” You can see here how many publications appear for each year, but here are some highlights:
2000: 2,063 articles (year I completed my dissertation study)
2024: 13,514 articles
2025: 21,477 articles
2026: 7,933 articles (so far, halfway through the year)
I don’t know about you, but I have some difficulty squaring up these physician complaints about being called “providers” when there is also a need for patients to be called by names that support their autonomy, expertise, and values.
This huge rise in studies using the term “patient compliance” is not pointing in that direction, disappointingly. It hearkens back to all those outdated presumptions about patients being compelled to follow medical directives.
This is about adherence and compliance, still, but so many other names and frames.
What do you notice about the differences between being a customer and a patient?
yours in solidarity✌️
Karen
In the late 1990’s nurses o know did a study where they personally administered a questionnaire to people with ESRD. The study structure was weak and loose and the data hung around for years, but in about 2003, we had an intern organize it and annotate other literature. We wrote it up and got an award in a nephrology nursing journal. We identified many barriers that affect compliance. Trusting the system and advisors was part of it, but (not in order) dosing schedule, side effects perceived or real, affordability, belief the treatment works or would for them, hassle factor (like 18 meds six different times a day-empty stomach, full stomach, between meals, ac, pc, hs, TIW, QM, etc.), ability to afford rent, child care, and premiums. Most people realized that the sanest response was non-compliance.
Hey Dr. Karen, you brought the heat, my friend!! I'm here for it!🙌🏽
I think this is where the language issue gets even bigger. The words "provider" and "patient compliance” are not separate problems in my mind. They are symptoms of the same machine.
The stealth use of the word "Provider” flattens physicians into interchangeable labor units, making it seem harmless because the person on the other side of the interaction doesn't stop to think about its impact, but it keeps them compliant, I mean, complacent in demanding better care.
"Compliance," on the other hand, flattens patients into people who are supposed to obey a plan, even when that plan may not fit their money, life, fear, history, access, or actual body because in the mind of the physician, the training has taught them, I mean us, to be like demagogues.
And while we debate the words, the real question is, who benefits from flattening both sides? Maybe the insurance companies benefit by denying health care to their clients. Or it could be the health systems that benefit from being allowed to purchase practices across specialties and other smaller hospitals, cancel contracts, and freeze out practices that don't fall in line to control the regional market. Or it could be private equity that swoops in to devour the providers—oops, I mean doctors—to make a fast buck, then suck the resources out of that system only to declare bankruptcy.
If the Medical Industrial Complex can keep physicians thinking of themselves as just “providers,” then clinical judgment can be scheduled, measured, rushed, and replaced. And if the MIC can keep a patient sick and tired and on the verge of bankruptcy, then they are judged by “compliance” measures, all while the burden of a failed plan quietly shifts onto the person who had the least power in designing it.
I keep coming back to in my observations.
1. Who decided a physician gets seven minutes with a patient?
2. Who decided the visit is structured that way?
3. Who decided the price is unknowable until after the care is delivered?
4. Who decided patients should enter one of the most expensive systems in American life without knowing what anything costs?
This did not happen by accident.
I've trained and practiced inside these systems. I've watched medicine become more corporate in real time. I've watched practices get absorbed. I've watched physicians become employees. I've watched clinical decisions get squeezed by workflows that were not designed around care.
So I do not think this is just semantics. Language is how the system trains people to accept their position inside it, right?
Patients get trained to wait.
Physicians get trained to produce.
And the people designing the rules stay unnamed.
That is the part we have to stop allowing.
If we are going to talk about language, we have to name the system using the language to protect itself.